



Regenerative Medicine Treatments for Tennis and Golfer’s Elbow

Overview of Tennis Elbow and Golfer’s Elbow
Overuse and repetitive contractions of the muscles and tendons of the forearm and elbow can put too much strain on the elbow tendons causing maladaptation’s in tendon structure that lead to pain.
Tennis Elbow (Lateral Epicondylitis) and Golfer’s Elbow (Medial Epicondylitis) are two of the most common elbow-related injuries. These injuries are often confused with each other but they are quite different and each affects different tendons in the elbow.
Tendons are a type of connective tissue made up primarily of strong collagenous fibers. However, they are not designed to stretch and extend. This makes the tendons in the elbow vulnerable to injury.
Indeed, elbow tendinopathy represents an important set of pathologies that account for lost recreation time, decreased quality of life, and work-related disability claims.
Who is at risk for developing Tennis Elbow and Golfer’s Elbow?
Both conditions can be the result of the sport for which they are named but a variety of activities can cause epicondylitis.
Tennis Elbow can result from any racquet sport but also professions including carpentry, painting, plumbing, cooking (cutting food), and repetitive computer mouse use.
Those at risk for Golfer’s Elbow include baseball pitchers, painters, and those whose professions involve gripping and twisting motions (e.g., repetitive screwdriver use). Pitchers and overhead throwing athletes often develop the disease because of high energy forces to the elbow during the late cocking and acceleration phase.
In golfers, it is thought to occur from the top of the backswing to just before ball impact. In tennis players, those using a one-handed backhand are at particularly at risk. One study reports up to 50% of all recreational tennis players will develop Tennis Elbow
Overall, epicondylitis affects 1-3% of the population, is more common in women and in those between 35-64 years old. Epicondylitis predominantly occurs on the lateral rather than on the medial side of the joint, with a 4:1 to 7:1 ratio.
Importantly, more than 90% of cases are not sports-related. In fact, in certain occupations, the prevalence of epicondylitis may be as high as 3.8% to 8.2%.
Obesity and smoking are considered independent risk factors for developing Tennis or Golfer’s Elbow.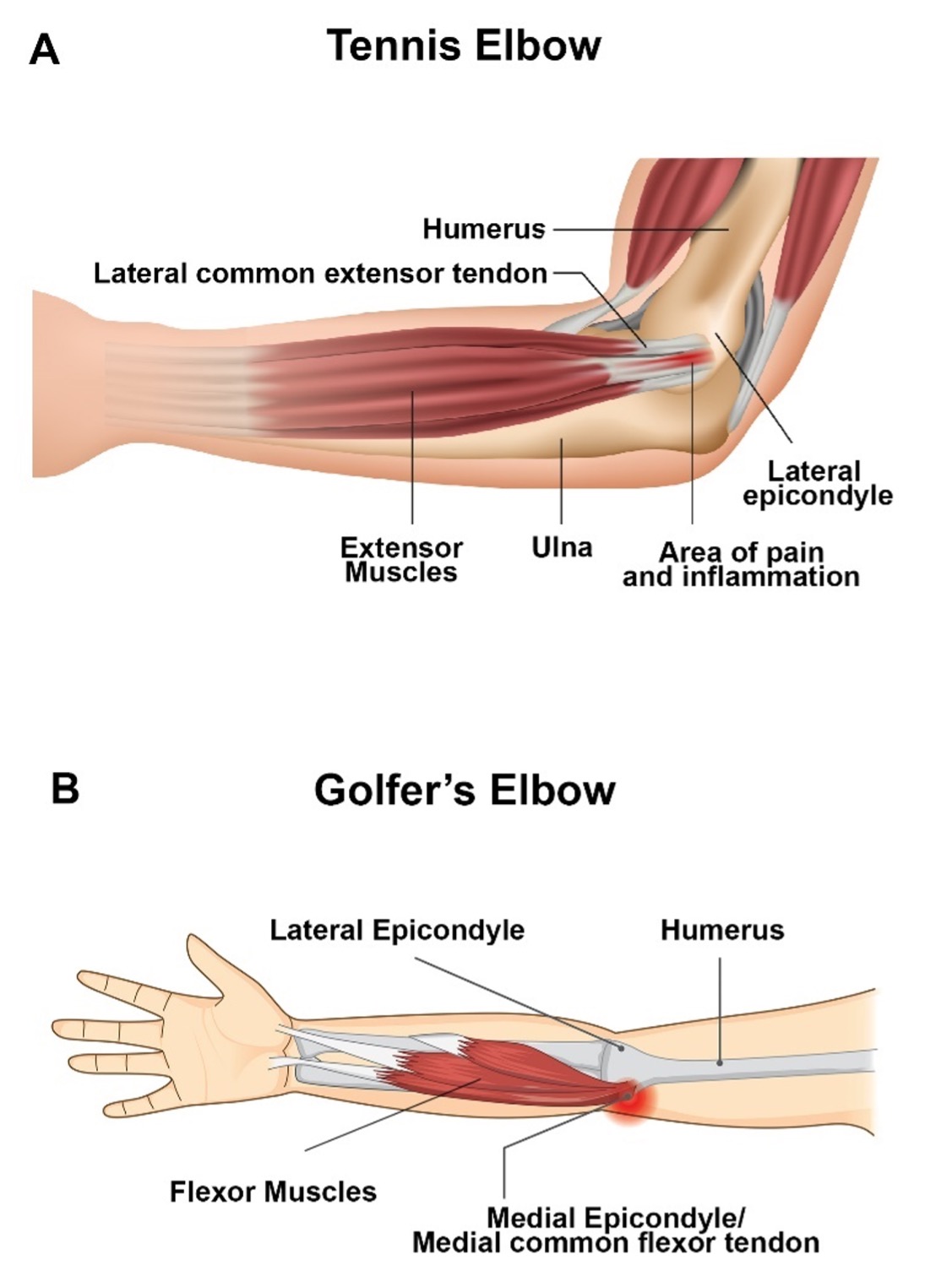
Symptoms of Tennis Elbow and Golfer’s Elbow
Generally, pain around the lateral and medial elbow differentiate Tennis Elbow from Golfer’s Elbow, respectively. However, in both cases the following symptoms may occur:
- Pain and tenderness that may radiate into the forearm and wrist that worsen with certain movements twisting, gripping, extension, or making a fist
- Weakness in the hands and wrists
- Stiffness in the elbow
- Numbness or tingling that might radiate into one or more fingers
With mild injury, both conditions may self-resolve, eventually disappearing when the activity causing the pain is ceased. However, these conditions can become chronic requiring intervention when the activity responsible for the injury continues over time.
Pathophysiology of Tennis Elbow and Golfer’s Elbow
Figure 1. Illustrations showing the muscles and tendons involved in epicondylitis. (A) dipicts lateral epicondylitis or Tennis Elbow whereas, (B) dipicts medial epicondylitis or Golfer’s Elbow.
The elbow joint is made up of three bones: the humerus (upper arm bone), the radius and ulna (two bones in the forearm). At the distal end of the humerus nearest the elbow, there are two epicondyles, one lateral (on the outside) and one medial (on the inside) (Fig. 1A, 1B). These are enlarged regions of the humerus where tendons connecting the muscles of the forearm attach to the humerus. The lateral and medial epicondyle is the common origin of the extensor and flexor muscles of the forearm, respectively.
Tennis Elbow involves injury to the common extensor tendon that originates from the lateral epicondyle of the elbow.
Several forearm muscles (the extensor carpi radialis brevis and longus, extensor digitorum, extensor digiti minimi, and extensor carpi ulnaris) come together to form the common extensor tendon (Fig. 1A). Repeated overloading of these muscles can lead to tendinopathy.
Golfer’s Elbow is tendinopathy of the medial common flexor tendon of the elbow. Together, the pronator teres, flexor carpi radialis, palmaris longus, and flexor digitorum superficialis form the common flexor tendon which originates from the medial epicondyle of the humerus (Fig. 1B).
In athletes, training errors, improper technique, equipment, or functional risk factors including lack of strength, endurance, or flexibility are all factors that can lead to lateral and medial epicondylitis. Inflammation and tearing of the tendons at the epicondyles are main cause of pain in Tennis and Golfer’s Elbow (Fig. 1A, 1B).
As mentioned above, it is the chronic repetitive loading of the forearm muscles and wrist that results in degeneration of the tendon due to decreased blood flow and damage to the collagenous fibers that make up the tendon.
Repetitive activity leads to recurrent microtears within the tendon and subsequent tendinosis. As the tendon undergoes repetitive microtears, there is remodeling of the collagen fibers, focal necrosis (tissue death) and calcification.
Subsequently, collagen strength decreases leading to increased fragility, scar tissue formation, and thickening of the tendon which causes significant and potentially debilitating pain. Although less common, acute trauma can also cause epicondylitis from a sudden violent contraction of the muscles.
Conventional Treatments for Tennis Elbow and Golfer’s Elbow
Tennis and Golfer’s elbow require medical attention as soon as the symptoms appear. Early attention usually prevents the development of a serious disorder.
The most important steps in treatment include:
- Rest from the activities that cause elbow pain
- Correction of incorrect technique, form, postures, and motions
- Medication such as oral or topical non-steroidal anti-inflammatory drugs (NSAIDS) to reduce the inflammation or pain
- Exercises to stretch and strengthen the muscles
- Physiotherapy to assess the healing process and restore the elbow function
- Corticosteroid (cortisone) injections (may have significant side effects)
Surgical Intervention for Tennis Elbow and Golfer’s Elbow
If these remedies fail to resolve the pain, then diagnostic imaging such as ultrasound or MRI may be used to determine if surgical intervention is needed to repair the damaged tendon.
Typically, 6-12 months of conventional treatment is undertaken before surgery is considered. The downtime from surgery is approximately 6-12 weeks. During this time exercises are recommended to restore range of motion and strength but 4-6 months are needed before exercise and sporting activities can be resumed.
Unfortunately, many patients do not return to their previous recreational sporting activities. Possible complications related to surgery are: infection, damage to nerves or blood vessels in the elbow, and reduced strength or flexibility.
ALSO READ: Regenerative Medicine: Non-Surgical Alternatives to Knee Surgery
Regenerative Medicine Treatments for Tennis Elbow and Golfer’s Elbow
The field of regenerative medicine has revolutionized the treatment of osteoarthritic and sports-related bone and joint injuries. Two regenerative medicine treatments have shown clinical efficacy: growth factor injections, and plasma rich platelet (PRP) injections.
A growing number of professional and amateur athletes are turning to regenerative medicine treatments before considering surgery. The advantages of advanced stem cell regenerative medicine treatments are:
- Little to no downtime due to the procedure
- Results can be boosted with physical therapy
- Avoid the side effects of pharmaceutical and cortisone drug therapies
- All-natural biological treatments help to avoid surgery
Growth Factor Injections
Growth factor injections work by stimulating resident cells to regenerate and heal the damaged tissue. These injections lower pain and reduce inflammation. The technique can be used to treat various sports-related injuries including Tennis Elbow and Golfer’s Elbow.
In a clinical study, amniotic protein fluid used in patients with tendonitis completely restored normal architecture of the tendon, and optimally aligned tendon fibers by stimulating the synthesis of matrix proteins such as type 1 collagen, hyaluronic acid, fibronectin and laminin.
Patients undergoing this personalized regenerative medicine treatment successfully gained complete mechanical strength and functionality of the tendon.
Growth factor injections are another approach and can be used in conjunction with allograft injections. Growth factors are naturally occurring proteins or hormones capable of stimulating cell proliferation, wound healing, and occasionally cellular differentiation.
Injection of growth factors into injured joints aid in the remodeling and repair of microtears in tendons associated with epicondylitis. When used with allograft injections they can accelerate the rate of healing.
Platelet Rich Plasma (PRP)
Platelet Rich Plasma (PRP) therapy also stimulates healing without pharmaceuticals. PRP begins with drawing some of the patient’s blood and processing it through the use of a high-speed centrifuge.
The concentrated platelets secrete at least seven different growth factors that promote healing and pain relief when injected into the affected area.
In chronic lateral epicondylitis, PRP therapy has been shown to effectively reduce pain and symptoms several short-term studies (reviewed by Taylor et al., 2012).
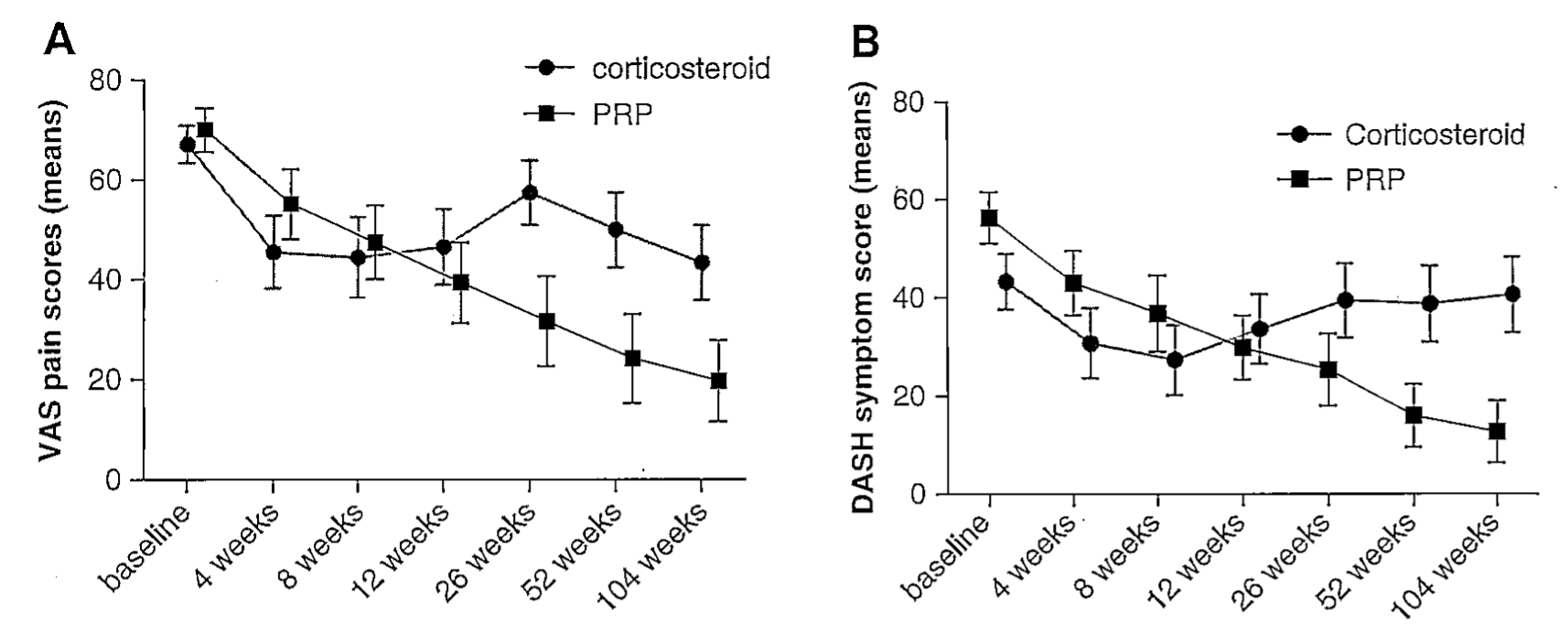
In a recent study, patients with chronic lateral epicondylitis were randomized to either PRP or corticosteroid injection treatment groups. Improved pain relief (Fig. 2A) and symptoms scores (Fig. 2B) in the PRP group were demonstrated at 1- and 2-years post treatment and were significantly better relative to the cortisone treatment group.
Figure 2. Platelet Rich Plasma (PRP) therapy vs. cortisone shot therapy in patients with lateral epicondylitis (Tennis elbow). A) Patients in the PRP therapy group reported significantly larger decreases in (A) pain and (B) related symptoms than patients treated by corticosteroids at 26, 52, and 104 weeks.
Recent Posts

BMI and Weight Loss: Understanding the Impact on Health
Body Mass Index (BMI) serves as a widely used tool for assessing weight status relative to height, offering valuable insights

Faqs About Regenerative Medicine and Stem Cell Treatment
Common-faqs-regenerative-medicines-and-stemcell-treatment

Five Habits that Could Be Worsening Your Knee Pain
Five Habits that Could Be Worsening Your Knee Pain

Cortisone Shots vs Regenerative Medicine Injections
Conventional treatments for joint pain often end up with long-term administration of cortisone shots, a powerful corticosteroid